
from the studio

A guide to the evidence behind sports recovery: from ice baths and massage guns to
infrared saunas and compression boots, and why the most important tools in your
arsenal probably don’t plug in.

AN ARTICLE BY ALLY TAYLOR
Walk into any high-end gym, scroll through your social feed for thirty seconds, or wander into a sports show, and you will be bombarded by what has become a multimillion-pound industry built around one idea: that recovering from exercise requires expensive intervention. Cryo chambers. Ice baths that cost more than a family holiday. Vibrating massage guns that look like power tools. Compression boots that make you resemble an extra from a science-fiction film. Infrared saunas promising to heat your muscles from the inside out while simultaneously detoxing your soul.
We are told that to be “optimal” we must spend almost as much time recovering as we do training, and that only these tools will get us there. Here is the confrontational truth: for most people, the recovery industry is selling them a very expensive way to polish a flat tyre.
That does not mean the tools are all useless. Some of them, used correctly and at the right time, do offer genuine, measurable benefit. The problem is that the marketing runs about ten years ahead of the science, and the science itself has become far more nuanced in the last few years than the brands would like you to know.
What follows is a plain-language guide to what the research actually shows, covering cold water immersion, infrared and photobiomodulation therapy, percussive massage guns, foam rolling, compression boots, blood flow restriction training, and wearables. We’ll look at what works, what doesn’t, when it matters, who it’s for, and just as importantly, who it isn’t for. To make the science more user friendly, we’ll follow two people: Frank, a 60-year-old keen cyclist who wants to keep riding strong, and Priya, a 34-year-old amateur runner currently building up to her first marathon while managing a desk job and two small children.
The Hierarchy: Why 95% of Your Results Come From the Boring Stuff
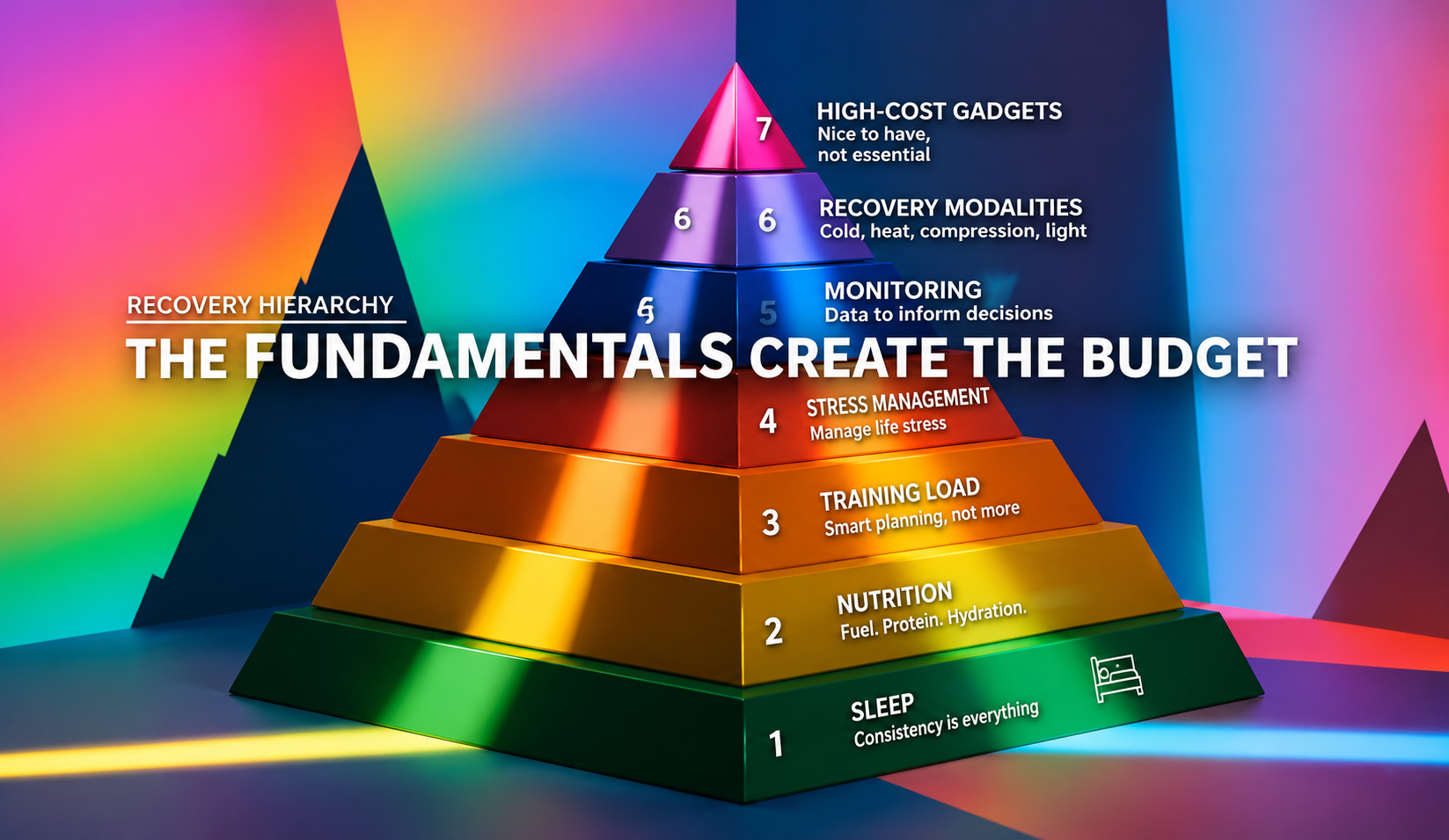
Before we get to the gadgets, we need to talk about the pyramid. The simplest way to think about recovery is this: your body has a recovery budget. The fundamentals, sleep, nutrition, and sensible training load, create that budget. Everything else mostly helps you spend it a little more wisely. If the budget is tiny because you’re sleeping five hours a night, eating poorly, and training without structure, then an ice bath is not “recovery.” It is just being cold and miserable for no measurable reason.
Sports scientists sometimes describe this as a hierarchy or pyramid, where the base layers must be adequately in place before the upper layers contribute meaningfully. A sports version of Maslow’s Hierarchy of Needs if you will. It is a coaching heuristic rather than a precise equation, but the underlying logic is solid: if your fundamentals are compromised, the marginal gain from any recovery modality shrinks towards zero.
Here is how the hierarchy looks in practice:
- Sleep consistency: Not just total hours, but regular bed and wake times. The evidence for sleep as the single most powerful recovery tool is overwhelming and almost entirely free.
- Nutrition: Adequate calories and sufficient protein (around 1.6–2.2g per kg of bodyweight per day for active adults), and carbohydrates to replenish glycogen. The Mediterranean style diet leads the way for healthful eating for most adults. No gadget compensates for a nutrition deficit.
- Training load management: Volume, intensity, and rest days that your body can absorb. Overtraining is not fixed by a massage gun, and nor is undertraining.
- Stress management: Systemic life stress raises cortisol, reduces recovery capacity, and increases baseline inflammation. A cold plunge does not undo a brutal work week.
- Monitoring and wearables: Useful for spotting trends and informing decisions, not for directly repairing tissue.
- Recovery modalities: Cold water immersion, heat, compression, photobiomodulation, and similar tools.
- High-cost gadgets: The expensive extras that are very easy to overvalue.
If you are not doing steps one to four consistently, jumping to step seven is like trying to fix a structural crack in your house by repainting the front door. You may feel better momentarily, but the house is still falling.
| A note on cost |
|---|
A good blackout blind and a consistent bedtime costs approximately £30. A home ice bath setup costs £200–500. A cryotherapy chamber session costs £50–100. A commercial infrared sauna costs £2,000–5,000. The evidence base for sleep dwarfs the evidence base for cryotherapy by several orders of magnitude. Spending order matters. |
Cold Water Immersion: The Double-Edged Sword

Cold water immersion (CWI) is the poster child of the modern recovery movement. Influencers take it. Former professional athletes evangelise it. Wellness brands have built entire product lines around it. The science, however, tells a more complicated story, one that depends critically on what you’re training for and when you apply it.
What it does: Immersing in cold water (generally defined as 10–15°C for 10–20 minutes) triggers vasoconstriction, reduces local inflammation, blunts the perception of fatigue, and can reduce delayed onset muscle soreness (DOMS). For acute recovery between training sessions or competition days, these effects are genuinely useful. A 2013 comprehensive review by Versey, Halson, and Dawson confirmed that immersion in 10–15°C water for 5–15 minutes appears most effective at accelerating short-term performance recovery.
The adaptation-blunting problem: Here is where it gets more nuanced and where most brands go quiet. If your goal is to get stronger or build muscle, regular post-exercise CWI may be working against you.
When you resistance train, the resulting inflammation and cellular stress is not just damage to be managed; it is the actual signal your body uses to initiate adaptation. Specifically, it activates the mTORC1 signalling pathway, which drives muscle protein synthesis and, over time, hypertrophy. Applying cold immediately after a resistance session partially suppresses this signal.
The landmark study by Roberts and colleagues found that CWI (10 minutes at approximately 10°C) after resistance training attenuated mTORC1 signalling and, over 12 weeks, produced significantly smaller gains in muscle mass compared to active recovery, roughly 2% versus 15% in quadriceps cross-sectional area. Subsequent research and meta-analyses have broadly supported this finding.
| What the evidence says |
|---|
| ✔ Good evidence Reduced perceived fatigue and DOMS between sessions and during multi-day events. Short-term performance recovery in endurance contexts (10–15°C, 10–15 minutes). Vasoconstrictive effects that reduce swelling and blunt soreness acutely. 🔵 Moderate evidence Perceptual benefits that appear independently of actual tissue-level recovery speed. Benefits from cold showers (less rigorously studied than full immersion). ❌ Weak or no evidence Building muscle or strength when used immediately post-resistance training. The evidence points in the opposite direction. Colder being proportionally better: the research supports 10–15°C, not increasingly extreme temperatures. |
Practical guidance: when matters more than whether
- After endurance exercise or multi-day events: CWI is genuinely useful. It reduces perceived fatigue and manages soreness so you can perform again the next day. Use it freely here.
- After resistance or hypertrophy training: avoid CWI in the 4–6 hours after your session if your goal is building strength or muscle. Wait until the evening if you must use it.
Recommended protocol: 10–15°C, 10–15 minutes. Shorter durations at colder temperatures are not better. They just feel more dramatic and more miserable.
| ✔ Frank’s take (60, keen cyclist) After a long ride, especially before another ride the next day, CWI is a legitimate tool in Frank’s kit. After gym sessions focused on leg strength, he should skip it. The cold plunge and the strength session are not the problem. Combining them is. |
| ✔ Priya’s take (34, marathon runner) In the weeks before her marathon, during high-mileage blocks where recovery between runs is paramount, CWI could genuinely help. During strength-building phases earlier in her programme, it’s better avoided. The timing matters far more than the tool. |
| ⚠️ Safety considerations CWI is not appropriate for everyone. Speak to your GP before starting if any of the following apply: Raynaud’s phenomenon or cold urticaria (cold allergy). Cardiovascular disease, uncontrolled hypertension, or a recent cardiac event. Pregnancy. Open wounds or active skin infections. Never plunge alone: cold shock response can cause sudden cardiovascular incapacitation. |
Infrared Therapy and Photobiomodulation: More Than a Red Glow

Infrared saunas and photobiomodulation (PBM) devices, which use red and near-infrared light directed at muscle tissue, are among the more legitimately interesting areas of recovery research, even if the consumer marketing around them tends to oversell significantly.
Unlike traditional saunas that primarily heat the air around you, near-infrared wavelengths (typically 800–900nm) penetrate the skin and interact with mitochondria in the muscle tissue, stimulating cytochrome c oxidase activity and influencing cellular energy production.
A comprehensive systematic review and meta-analysis by Leal-Junior and colleagues found that photobiomodulation therapy, particularly when applied before or after exercise using red or near-infrared wavelengths, reduced markers of muscle damage, attenuated creatine kinase elevations, and improved performance maintenance in subsequent efforts. The most consistent results came with pre-exercise application, where PBM appeared to act as a kind of cellular warm-up.
For practical purposes, this translates to potentially feeling less stiff, recovering neuromuscular function slightly faster, and experiencing reduced DOMS after intense sessions. The effect is real but very modest; it is unlikely to substitute for sleep or nutrition or a nice walk in the fresh air.
It is also worth separating what infrared saunas and PBM devices do from what they are marketed as doing. Many consumer infrared saunas are used primarily at temperatures too low and for durations too short to deliver meaningful tissue-level photobiomodulation. The relaxation effect is real, and the mild cardiovascular stimulus from heat exposure has its own literature. But “detoxing your cells” is not a biological process that exists in any meaningful clinical sense.
| What the evidence says |
|---|
✔ Good evidence Reduced markers of muscle damage, including creatine kinase elevations, in clinical studies.Reduced DOMS in some populations, particularly with pre-exercise application.Pre-exercise PBM appears to act as a cellular primer, improving subsequent performance maintenance. 🔵 Moderate evidence. Short, low-temperature sauna sessions producing meaningful photobiomodulation at the tissue level.Cardiovascular benefits from regular heat exposure (a separate evidence base with its own modest literature). ❌ Weak or no evidence “Cellular detox” as a biological mechanism. This is not how cells or detoxification work. |
For most people, if the sauna makes you feel better, more relaxed, and more likely to sleep well afterwards, that is itself a legitimate recovery outcome. Just do not expect it to compensate for a poor night’s sleep.
| ✔ Frank’s take (60, keen cyclist) If Frank has access to an infrared sauna and it helps him wind down after a training block and sleep better, that is a legitimate use. He should not expect it to compensate for a week of poor rest or fix a training load that is too high. Pre-session light therapy from a clinical-grade device may modestly reduce DOMS. Useful. Not transformative. |
| ✔ Priya’s take (34, marathon runner) Priya’s recovery budget is constantly being raided by life stress. A hot sauna, or even a warm bath, that gets her parasympathetic nervous system to switch on and delivers her to sleep faster is doing some recovery work, even if it is not the photobiomodulation the brochure promises. The relaxation effect alone earns its place. |
| ⚠️ Safety considerations Most quality PBM research uses clinical-grade devices with precise wavelength and dosing parameters. Consumer products vary enormously. Avoid PBM directly over areas with active cancer, during pregnancy, or over the thyroid gland. Infrared saunas carry the same cardiovascular cautions as traditional saunas. If you have heart disease or low blood pressure, speak to your GP first. Stay hydrated: heat-related dehydration is a genuine risk with prolonged sauna use. If you feel dizzy, nauseous, or faint, get out. The body is not a slow cooker. |
Percussive Therapy and Foam Rolling: The Neurological Nudge

Everyone has seen someone at the gym methodically punishing their quads with a percussion massage gun while wearing the expression of someone contemplating a complex philosophical problem. Does it help?
The honest answer is: somewhat, for specific things, for a short period of time. The 2019 meta-analysis by Wiewelhove and colleagues, the most comprehensive quantitative synthesis on foam rolling to date, found small but meaningful effects on short-term range of motion and subjective muscle soreness, with minimal evidence of lasting structural change to muscle tissue. More recent work on percussive devices specifically found broadly similar results: they appear to work through the same neurological mechanisms as foam rolling, and the choice between them is largely one of preference and practicality.
The mechanism is primarily neurological rather than structural. Rolling or percussive stimulation appears to temporarily reduce pain signalling and increase stretch tolerance, what researchers call a change in “stretch perception” rather than a change in the actual properties of the tissue. This is why the popular claim that massage guns “break up fascia” is nonsense. Meaningful changes to fascial architecture require either sustained load of more than one tonne over time, or a surgeon’s scalpel. A hand-held vibrating device cannot do this, and the marketing that implies otherwise should be treated with the same scepticism as any other unsubstantiated health claim.
It also misunderstands what fascia actually is. Fascia is not a substance that overgrows; it is a connective tissue that wraps and runs through every single muscle in the body. Next time you break the leg off a whole chicken, the filmy stuff that gets thinner until it breaks: that’s fascia.
The ROM gains from a single session of foam rolling or vibration are real but time-limited. Most studies show the effects dissipate within 10–20 minutes. This makes them genuinely useful as part of a warm-up or to manage stiffness before a session, but less impressive as a post-workout recovery tool on their own.
| What the evidence says |
|---|
✔ Good evidence Short-term range of motion gains lasting approximately 10–20 minutes. Subjective soreness relief after training. Warm-up benefit when used before training to improve movement quality. 🔵 Moderate evidence. Meaningful acceleration of actual muscle repair. Evidence exists in some contexts but is modest. Benefits lasting beyond 20 minutes post-session when done regularly. ❌ Weak or no evidence “Breaking up fascia” or producing any structural remodelling of tissue. The biology does not support this. |
| ✔ Frank’s take (60, keen cyclist) Two minutes on the foam roller or massage gun targeting stiff hips and quads before Frank’s rides is practical sense if he has time available. After a long ride, it might take the edge off soreness and feel like earned self-care. He should use it at a pressure that feels therapeutic rather than punishing, and never aggressively on tissue that is already fatigued from a hard effort. |
| ✔ Priya’s take (34, marathon runner) A short foam rolling session before a morning run, when Priya is stiff from sitting at a desk all day, is potentially useful for getting her ready to move, but no more than some mobility or dynamic stretches, or even starting with a walk! After a hard session, it might reduce the feeling of soreness. The key word is feeling: the underlying repair still takes the same amount of time regardless of how many passes she does. |
| ⚠️ Safety considerations *These tools are low risk when used sensibly. Used aggressively, they can cause harm. *Avoid use directly over joints, bones, the front of the neck, open wounds, bruised tissue, and varicose veins. *Work at a pressure that feels like a 3–4 out of 10 discomfort. Not a challenge to endure. *If you notice a temporary reduction in ROM after use rather than an increase, stop. *Foam rolling for longer than approximately 60 seconds per muscle group before training can reduce explosive power output in some individuals. Keep pre-training sessions short. *Never use a percussion device on someone else without appropriate training, and never over tissue that has had recent surgery or acute injury. *A 2021 case report documented rhabdomyolysis following aggressive percussion device use on a fatigued athlete. Rare, but a useful reminder: more is not better. |
Compression Garments and Blood Flow Restriction: Two Very Different Things
These two modalities are often grouped together because both involve applying pressure to the limbs. They have almost nothing else in common.
Compression boots (intermittent pneumatic compression)

Those giant inflatable trousers that athletes sit in while scrolling their phones. Do they actually do anything? A 2024 systematic review and meta-analysis found trivial to small benefits for lower-limb intermittent pneumatic compression on perceptual recovery and soreness, and slightly better effects on creatine kinase (a marker of muscle damage) at 48 hours post-exercise. The mechanism is largely mechanical: the sequential inflation promotes lymphatic drainage and venous return, which helps clear metabolic waste from the tissues.
The practical value, as with CWI, is primarily perceptual: you feel less heavy-legged and less sore. For Frank after a 60-mile ride, they are a legitimate end-of-session comfort ritual. The important clinical caveat is that feeling less sore does not mean you are fully recovered. The perception of soreness is blunted, but the underlying muscle repair timeline is largely unchanged. Going out hard again too soon because “I feel fine” is a genuine overtraining risk.
| What the evidence says |
|---|
✔ Good evidence Perceptual recovery, meaning feeling less heavy-legged and less sore after endurance sessions. Modest effects on creatine kinase (muscle damage marker) at 48 hours post-exercise. Promotion of lymphatic drainage and venous return via sequential mechanical compression. 🔵 Moderate evidence. Reliable performance benefits in the session immediately following use. ❌ Weak or no evidence Perceived soreness as a trustworthy indicator of full recovery after compression boot use. The blunting effect means you may feel better than you actually are. Meaningful acceleration of actual muscle repair timelines. Perception improves more than the underlying biology. |
| ✔ Frank’s take (60, keen cyclist) After a 60-mile ride, especially before another ride the next day, compression boots are a nice comfort ritual for Frank. He should enjoy the feeling of lighter legs without taking it as a green light to train hard the following morning if the session was highly demanding. Feeling better is not the same as being recovered. |
| ✔ Priya’s take (34, marathon runner) After a long Sunday run in her marathon build, 20–30 minutes in compression boots, or a pair of compression shorts on the commute home, would take the edge off heavy legs. The same caveat applies equally to her: feeling better does not mean she is ready for another hard session. Use the perceptual benefit without letting it override sensible training logic. |
| ⚠️ Safety considerations *Compression boots are generally safe for healthy adults. Avoid or seek medical advice if you have: *Peripheral arterial disease or poor lower-limb circulation. *Deep vein thrombosis (DVT) or a history of clotting disorders. *Active skin infections or open wounds on the lower limbs. *Significant oedema of unknown cause. *If in doubt, check with your GP before use. |
Blood Flow Restriction (BFR) Training
BFR is an entirely different proposition, and one with strong evidence for specific populations. It involves applying an inflatable cuff to the proximal aspect of a limb during low-load resistance exercise, partially restricting venous outflow without fully occluding arterial inflow. This creates a local hypoxic environment that tricks the body into responding as if the load is much heavier than it is, producing meaningful muscular adaptation at loads as low as 20–30% of one-repetition maximum.
A systematic review and meta-analysis in Sports Medicine found that low-load BFR training produced comparable gains in muscle mass and strength to conventional high-load resistance training in older adults. For anyone managing joint pain, recovering from surgery, or simply unable to tolerate heavy loading, this is clinically significant. The broader methodology and safety framework for BFR practice was outlined by Patterson and colleagues.
| What the evidence says |
|---|
✔ Good evidence Comparable muscle and strength gains to high-load training at loads as low as 20–30% of 1RM. Strong evidence specifically in older adults and those with joint limitations who cannot tolerate heavy loading. Clinically meaningful results in rehabilitation contexts, including post-surgical recovery. 🔵 Moderate evidence. Benefits in otherwise healthy, pain-free athletes as a primary training method. Evidence exists but is less compelling than for special populations. ❌ Weak or no evidence Self-prescribed BFR without limb occlusion pressure measurement being safe or effective. Cuff pressure must be individualised, not guessed. |
| ✔ Frank’s take (60, keen cyclist) With knee pain preventing Frank from squatting heavy, BFR with light loads under professional guidance could allow him to maintain leg strength without joint stress. This is one of the most evidence-backed tools in this document for his specific situation. He should not self-prescribe it. The cuff pressure needs to be properly calibrated. |
| ✔ Priya’s take (34, marathon runner) If Priya develops knee or hip pain during her marathon build (very common), BFR training under professional guidance could allow her to maintain strength in the affected area at much lower loads. This is not a DIY tool. It requires proper assessment and cuff pressure calibration. Done correctly, it could be the difference between managing through a niggle and having to abandon her training block. |
| ⚠️ Safety considerations BFR requires professional supervision for these groups: *Uncontrolled hypertension or significant cardiovascular disease. *History of deep vein thrombosis (DVT) or clotting disorders. *Sickle cell trait or other haematological conditions. *Pregnancy. Cuff pressure must be individualised using limb occlusion pressure (LOP) measurements, not guessed. Do not self-prescribe BFR without proper assessment. |
Wearables, HRV, and the “Decision Support” Problem
Wearables: HRV monitors, sleep trackers, readiness scores and strain metrics, occupy a peculiar position in the recovery ecosystem. They do not recover you. They do not repair tissue, restore glycogen, or calm an overactivated nervous system. What they can do, used intelligently, is help you make better decisions about training load.
Heart rate variability (HRV), the variation in time between successive heartbeats, is the most scientifically validated of the wearable metrics. Consistently low or declining HRV across several days correlates with accumulated fatigue and reduced readiness to train hard. A single day’s reading is largely noise; the trend over five to ten days is the signal.
The risk with wearables is that people outsource their body awareness to an algorithm. If your device says “recovery score: 94%” but you feel genuinely exhausted, your body is right and the algorithm is wrong. These tools are decision support. They do not override clinical judgement, coaching wisdom, or the person living in the body in question.
AI-driven recovery platforms are beginning to emerge, promising hyper-personalised training prescriptions based on continuous physiological data. The concept is interesting. The current reality is that no algorithm yet available to consumers reliably outperforms an experienced coach working with a responsive athlete. This space is worth watching, but not worth reorganising your training around.
A practical note: if you find that checking your recovery score first thing in the morning makes you anxious, you have inverted the point of the tool. It should reduce uncertainty, not create it.
| What the evidence says |
|---|
✔ Good evidence HRV trends over 5–10 days correlate meaningfully with accumulated fatigue and training readiness. Wearable data can help identify overreaching before the athlete is consciously aware of it. 🔵 Moderate evidence. Consumer sleep staging data, where accuracy varies significantly from clinical polysomnography. Single-day readiness scores as reliable training prescriptions. ❌ Weak or no evidence Current AI recovery platforms reliably outperforming experienced coaches working with responsive athletes. Any wearable metric substituting for the direct experience of living in your body. |
| ✔ Frank’s take (60, keen cyclist) A basic HRV tracking app would tell Frank something useful if his scores are consistently low across a week: he is probably carrying more fatigue than he realises. It will not tell him anything his legs couldn’t tell him if he paid attention. The risk for Frank, as with many data-oriented people, is that a high readiness score overrides his body’s genuine signals to take it easy. |
| ✔ Priya’s take (34, marathon runner) Priya’s readiness score the morning after four hours of broken sleep with a sick toddler is not going to say anything she does not already know. A wearable that adds guilt about her HRV on top of everything else she is managing is not a recovery tool; it is another source of stress. Used as a broad trend tracker rather than a daily verdict, it might help her spot when marathon training is accumulating too fast. |
| ⚠️ Safety considerations Minimal physical safety concerns. The real risks with wearables are psychological: *Anxiety from daily readiness scores displacing actual body awareness. *Using a high readiness score to justify training through genuine fatigue. *Over-reliance on device data at the expense of coaching input and self-knowledge. *If your device is adding to your stress rather than reducing it, turn off the daily notifications. Or put it in a drawer for a week and notice whether training feels any different. |
The Psychology of Recovery: The Dimension the Industry Ignores
Almost no recovery marketing mentions the psychological dimension, which is unfortunate because it is one of the most robustly supported aspects of the whole enterprise.
Recovery modalities that involve deliberate rest, warmth, calm environments, and sensory experience: saunas, massage, even ice baths if you find them energising, activate the parasympathetic nervous system. This shift from sympathetic (“fight or flight”) to parasympathetic (“rest and digest”) activity is itself a type of recovery mechanism. Cortisol drops, heart rate variability improves, and the perception of readiness increases. These benefits fall into the bracket of placebo effects, which is not to dismiss them; they are real physiological shifts with potentially meaningful consequences for subsequent performance.
The ritual of recovery also matters psychologically. Having a deliberate wind-down protocol after training, whether it is five minutes of foam rolling, a hot shower or ten minutes of quiet, creates a clear psychological transition from the training state to the recovery state. For athletes managing high life stress, this transition can be a helpful adjuvant.
| What the evidence says |
|---|
✔ Good evidence Parasympathetic activation via deliberate rest, warmth, and calm environments reduces cortisol and improves HRV. Placebo effects from recovery rituals are real, measurable physiological responses. Not imaginary, but not effective for the reason the marketing gave. 🔵 Moderate evidence. Specific protocols (sauna vs bath vs foam rolling) having meaningfully different psychological recovery effects in healthy adults.. ❌ Weak or no evidence Any specific consumer product being necessary for psychological recovery. The mechanism is parasympathetic activation, not the product delivering it. |
| ✔ Frank’s take (60, keen cyclist) Frank’s post-ride routine, whether it is a long shower, a good meal or ten minutes of just sitting quietly, is itself doing recovery work. The neurological shift away from effort mode matters. If the ritual also involves checking five biometric apps and worrying about his power data, it undermines the whole point. The transition is the thing. |
| ✔ Priya’s take (34, marathon runner) Priya’s most useful psychological recovery tool might simply be a defined boundary between training time and everything else. Fifteen minutes of deliberate wind-down that belong entirely to her, not the job, not the children, creates the mental transition that allows recovery to actually begin. This costs nothing except the decision to protect the time. |
| ⚠️ Safety considerations *The main psychological risk in recovery practice is anxious monitoring: when tools designed to reduce uncertainty become a source of it. *If recovery rituals are creating pressure, obligation, or guilt rather than rest, they are doing the opposite of their job. *A recovery practice that adds stress is not a recovery practice. There is no obligation to perform recovery in any particular way. |
How to Actually Recover: A Practical Guide
The fundamentals (non-negotiable)
- Sleep: Aim for 7–9 hours with consistent bed and wake times. If you are getting five hours, a Theragun will not compensate. Blackout curtains, a cool room, and screens off an hour before bed will.
- Protein: 1.6–2.2g per kg of bodyweight per day for active adults. This does not require supplements. Most people can reach adequate intake from food. A chicken breast, two eggs, some Greek yoghurt, and a handful of nuts across the day go a long way.
- Active recovery: A 20-minute walk, gentle swimming, or easy cycling between sessions promotes blood flow without adding stress. Total rest is often not the optimal choice, especially for DOMS.
Quick-reference guide: the tools
| Tool | Best Use | Avoid After | Practical Dose |
|---|---|---|---|
| Cold water immersion | Between sessions / multi-day events | Post-resistance / hypertrophy session | 10–15°C, 10–15 mins |
| Infrared / PBM | Stiffness, pre-session prep, relaxation | Not a substitute for sleep or nutrition | Device-dependent; follow manufacturer guidance |
| Massage gun / foam roller | Pre-session warm-up, short-term soreness relief | Aggressive use on fatigued tissue | 2–5 mins per area at 3/10 pressure |
| Compression boots | Post-endurance session, heavy legs | Don’t use feeling-better as a green light to overtrain | 20–30 mins as a comfort ritual |
| Blood flow restriction | Joint-limited strength training | Cardiovascular / clotting conditions | Requires professional set-up and LOP measurement |
| What the researchers would tell you |
|---|
The most consistent finding across the recovery science literature is the supremacy of the fundamentals. The studies that show meaningful effects from modalities like CWI and PBM are overwhelmingly conducted in populations who are already sleeping, eating, and training well. The marginal gains from adjunct tools are real but small. The marginal gains from fixing sleep are large and consistent across every population studied. This does not make the tools pointless. It means using them in the right order. |
The Bottom Line

The recovery industry is not a scam. Well, not entirely. Some of its tools have real, evidence-backed effects. But the industry has a fundamental incentive to frame those tools as more central than they are, and to convince you that the cherry on top is the cake.
For Frank, the most important recovery investment is consistent sleep, adequate protein, and a periodised training plan that does not accumulate load faster than his 60-year-old physiology can absorb. A cold plunge after his long rides and BFR work for his knees under professional guidance are useful additions, in that order and at that priority.
For Priya, juggling marathon training with a full life, the most powerful recovery tool is probably a consistent 10pm bedtime and a meal with enough protein in it. A massage gun before her morning runs and 20 minutes of deliberate wind-down after her hard sessions would add some value. A £3,000 gym membership just for the infrared sauna would not.
The best recovery protocol is not the most elaborate or expensive one. It is the one you will actually do, consistently, without adding so much complexity that the optimisation becomes the stressor. Do the fundamentals savagely well. Add the fun stuff as the cherry on top. And the next time someone tries to sell you a second mortgage’s worth of recovery kit, ask them how well you’d do with the same money spent on a better mattress, a good coach, and the goldilocks of training volume.
Ready to train the way the science actually suggests? [Start with an intro pack at Amovida.]
Bibliography
Readers are encouraged to access the primary literature directly.
Centner, C., Wiegel, P., Gollhofer, A., & König, D. (2019). Effects of blood flow restriction training on muscular strength and hypertrophy in older individuals: A systematic review and meta-analysis. Sports Medicine, 49(1), 95–108. https://doi.org/10.1007/s40279-018-0994-1
Chen, J., Zhang, F., Chen, H., & Pan, H. (2021). Rhabdomyolysis after the use of percussion massage gun: A case report. Physical Therapy, 101(1), pzaa199. https://doi.org/10.1093/ptj/pzaa199
Leal-Junior, E.C.P., Vanin, A.A., Miranda, E.F., de Carvalho, P.T., Dal Corso, S., & Bjordal, J.M. (2015). Effect of phototherapy (low-level laser therapy and light-emitting diode therapy) on exercise performance and markers of exercise recovery: a systematic review with meta-analysis. Lasers in Medical Science, 30(2), 925–939. https://doi.org/10.1007/s10103-013-1465-4
Li, H., Luo, L., Zhang, J., Cheng, P., Wu, Q., & Wen, X. (2025). The effect of percussion massage therapy on the recovery of delayed onset muscle soreness in physically active young men, a randomized controlled trial. Frontiers in Public Health, 13, 1561970. https://doi.org/10.3389/fpubh.2025.1561970
Maia, F., Nakamura, F.Y., Sarmento, H., Marcelino, R., & Ribeiro, J. (2024). Effects of lower-limb intermittent pneumatic compression on sports recovery: A systematic review and meta-analysis. Biology of Sport, 41(4), 263–275. https://doi.org/10.5114/biolsport.2024.133665
Patterson, S.D., Hughes, L., Warmington, S., et al. (2019). Blood flow restriction exercise: considerations of methodology, application, and safety. Frontiers in Physiology, 10, 1332. https://doi.org/10.3389/fphys.2019.01332
Petersen, A.C., & Fyfe, J.J. (2021). Post-exercise cold water immersion effects on physiological adaptations to resistance training and the underlying mechanisms in skeletal muscle: A narrative review. Frontiers in Sports and Active Living, 3, 660291. https://doi.org/10.3389/fspor.2021.660291
Roberts, L.A., Raastad, T., Markworth, J.F., Figueiredo, V.C., Egner, I.M., Shield, A., Cameron-Smith, D., Coombes, J.S., & Peake, J.M. (2015). Post-exercise cold water immersion attenuates acute anabolic signalling and long-term adaptations in muscle to strength training. The Journal of Physiology, 573(14), 4285–4301. https://doi.org/10.1113/JP270570
Versey, N.G., Halson, S.L., & Dawson, B.T. (2013). Water immersion recovery for athletes: effect on exercise performance and practical recommendations. Sports Medicine, 43(11), 1101–1130. https://doi.org/10.1007/s40279-013-0063-8
Wiewelhove, T., Döweling, A., Schneider, C., Hottenrott, L., Meyer, T., Kellmann, M., Pfeiffer, M., & Ferrauti, A. (2019). A meta-analysis of the effects of foam rolling on performance and recovery. Frontiers in Physiology, 10, 376. https://doi.org/10.3389/fphys.2019.00376
Be The First To Comment