
from the studio

The Biological Imperative of Strength: Why Margaret Started Lifting
Ally Taylor
02/03/2026

AN ARTICLE BY ALLY TAYLOR
Margaret is 65. She is not frail. She is not inactive. She does not consider herself old, and if you call her “elderly,” she will give you a look that suggests you should immediately reconsider your life choices.
She walks most mornings. Proper walks: brisk enough to feel virtuous, but not so brisk that she can’t talk. She gardens. She carries her own shopping. She refuses help with tasks on principle and will even lift her own suitcase into the overhead bin on a plane. She is, by most reasonable standards, doing well.
BUT…
The stairs at the train station feel longer than they used to. Getting up from the floor after playing with her grandson now involves a nearby chair and what can only be described as a “multi-point negotiation.” Lifting her suitcase into the overhead bin on the plane is possible, but in no way elegant.
No injury. No fall. Small but noticeable changes creeping in. She hasn’t told anyone this, but she has wondered to herself: “Is this just age?”
When someone suggests strength training, she laughs out loud. That’s for gym people. 20-year-olds in Sweaty Betty leggings and crop tops. For people who say “smash it” without irony. She walks. She stretches. She eats sensibly. Surely that’s enough?
This is where Margaret’s story meets physiology and science.
The Insidious Erosion
From our late forties onwards, women begin to lose muscle mass at roughly one to two percent per year. After menopause, that loss can accelerate as oestrogen declines. The process is gradual, which makes it easy to ignore. There is no fanfare. No siren. Just insidious erosion, like the melting of the polar icecaps – a little bit year-on-year which accumulates over decades to a global disaster.
The medical term is sarcopenia. Margaret does not need the word. She feels it in the stairs.
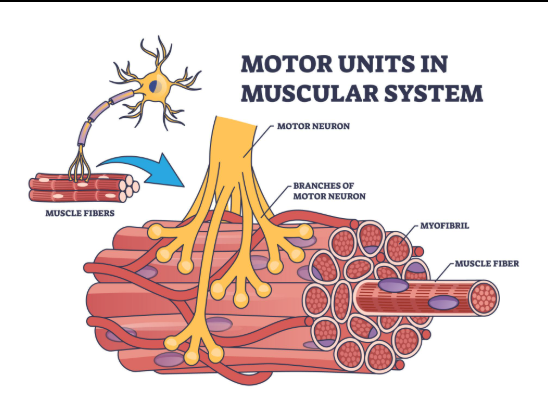
But sarcopenia is not just muscles getting smaller. It is about what muscle loss means for balance, coordination, metabolic diseases like diabetes, and fall risk. Inside every muscle are motor units; a motor nerve and the muscle fibres it controls. When you decide to stand up, your nervous system recruits motor units in an orderly fashion, from low-threshold units (good for gentle, sustained activity like walking) to higher-threshold units. These high-threshold units are responsible for stronger, faster contractions: jumping, throwing, stopping yourself from falling, and moving that suitcase!
With ageing, several things happen. We lose muscle fibres, particularly fast-twitch (Type II) fibres that help us move quickly and powerfully. The motor neurons that once controlled them may die back. Surviving neurons sometimes reinnervate “orphaned” fibres, but the overall system becomes less efficient.
Motor unit firing rates can slow down. Coordination can become less “coordinated.” In practical terms, this means that even if you still “have muscle,” your ability to recruit it quickly and effectively may decline. It’s like having the same hardware but the software has switched from high-speed fibre Wi-Fi to the property to old-school dial-up.
The Threshold for Adaptation
At the same time, muscle protein synthesis (the process by which the body repairs and builds muscle tissue) becomes less responsive. This is sometimes referred to as anabolic resistance. The same stimulus that built muscle at 30 may not be sufficient at 60. The threshold for adaptation is slightly higher.
This is one reason light, token resistance work often fails to move the needle in later decades. The stimulus must be strong enough to overcome that blunted sensitivity.
When you lift weights at sufficient intensity, mechanical tension is generated within the muscle fibres. That tension is sensed by molecular pathways inside the cell, which activate signalling cascades (including mTOR pathways) that increase muscle protein synthesis. In simple language: lift something challenging, and your muscle receives the message that it needs to adapt. If the message is too quiet, nothing much changes.

Why Walking Isn’t Enough for Your Bones
At a routine appointment, Margaret’s GP mentions osteopenia. It is not osteoporosis, but it is a warning sign. She is advised to keep walking, perhaps with a weighted vest or some weighted bangles to “add a bit more load.”
Let’s break this down using physiology. Weighted vests have their place. If you are training for a trek or preparing to carry a backpack across actual hills for actual miles, they are sensible. They increase metabolic demand. The heavier the vest, the harder your heart and lungs work. That is useful, depending on the goal.
But unless you are strapping on military-grade packs and marching for hours, the mechanical strain through the hip and spine is unlikely to approach the stimulus provided by progressive resistance training. A two- or three-kilo vest on a flat pavement walk does not replicate the compressive and tensile forces generated by a properly loaded squat or deadlift.
Bones respond to load. In the nineteenth century, Julius Wolff observed that bone architecture changes in response to the stresses placed upon it. Wolff’s Law describes the principle that bone remodels according to mechanical demand, along lines of stress. Modern physiology explains this through mechanotransduction. When bone tissue experiences sufficient stress, cells within the bone detect it and trigger signalling pathways that stimulate bone formation. Not enough stress = no signal = limited or no new bone growth.
This is where the LIFTMOR trial changed the narrative for women in menopause. For years, women with low bone density were advised to keep exercise light and avoid heavy lifting. The intention was safety. The unintended consequence was under-stimulation and increased frailty.
The LIFTMOR randomised controlled trial involved postmenopausal women with osteopenia and osteoporosis undertaking high-intensity resistance and impact training under supervision. Importantly, the loads were challenging at +80% 1 repetition max (1RM). The results showed clinically meaningful improvements in bone mineral density at the lumbar spine and femoral neck (hip) alongside improvements in strength and physical function.
Muscle: The Body’s 24/7 Factory
Muscle is not just decorative tissue. It is also protective infrastructure. It is the body’s largest site for glucose disposal. When you eat carbohydrates, your skeletal muscle helps regulate blood sugar. Less muscle means less metabolic buffer. That midlife figure change many people notice, where weight distribution shifts to a bit more around the middle, is not simply about willpower. It is also about tissue.
Muscle also behaves like an endocrine organ. It releases signalling molecules that influence inflammation, immune function, brain health, and cardiovascular risk. When muscle contracts, it sends helpful messages throughout the body. In that sense, strength training is not just about force production. It is about systemic resilience.
Then there is function: Standing up from a chair, climbing stairs, catching yourself when you trip, and carrying shopping without dividing it into “diplomatic parcels!”
Power and The Fear of Falling
Margaret hasn’t fallen. But she has seen friends fall. She has seen how quickly confidence evaporates after a fracture. Recovery is not just physical; it is psychological. What the fall steals from you is your confidence as you shrink your world for fear of falling again.
Falls are rarely about clumsiness alone. They are often about the interaction between strength, speed, balance, and the nervous system. When you trip, there is a chain of events that must happen very quickly:
- Sensory receptors in your feet detect the perturbation.
- Signals travel to the spinal cord and brain.
- The brain processes the information and sends rapid motor commands back to the muscles.
- Muscles produce force fast enough to reposition the body’s centre of mass.
If any part of that chain is slower or weaker, the correction may fail. Because we lose fast-twitch fibres more rapidly as we age, our “Rate of Force Development” decreases. This is why we train Power. Power is force multiplied by velocity. It is not just how strong you are, but how quickly you can express that strength.

Debunking the Myths
Let’s put these common myths to bed:
- Myth 1: “I’ll bulk up like a bodybuilder.”
Muscle hypertrophy requires mechanical tension, metabolic stress, and a specific hormonal environment: specifically testosterone. Post-menopausal women have testosterone levels approximately 5-10% of their male counterparts. You won’t look like a bodybuilder; you’ll look like a more defined, capable version of yourself. - Myth 2: “I’m too fragile for heavy weights.”
Avoidance of load does not protect tissue. Adaptation does. The key is proper progression. You don’t start with a 100kg barbell; you start with what is challenging for you today. - Myth 3: “I’ll hurt myself.”
Amovida prioritises clear technique before heavier load. Properly prescribed resistance training is safer than the alternative: becoming too weak to move safely in the world.
The Rebellious Act
Margaret began cautiously. She learned to squat to a box. She learned to hinge. She rowed. She pressed light dumbbells overhead and was surprised at how quickly her shoulders fatigued. Two sessions became three. Load increased slowly. Confidence increased.
Six months pass. She stands taller. She walks with less hesitation. She carries her shopping in one trip. She lifts her suitcase without commentary. She gets down on the floor with her grandson and stands up again without choreography. Her reflection has not transformed dramatically, but her capacity has.
At her doctor’s follow-up appointment, her bone density has stabilised, her strength has improved, and her metabolic measures are shifting in the right direction. None of this is miraculous. It is physiological.
There is a cultural script suggesting women over sixty should shrink, slow down, and accept decline politely. Strength training refuses that script. It builds infrastructure: Muscle, Bone, Balance, and Power.
Margaret never set out to be radical. She set out to remain capable. If you are wondering whether strength training is for you, the question isn’t whether you can lift weights. The question is whether you would like your seventy-five or eighty-five-year-old self to be independent. Margaret decided she would. She became prepared. And in the grand scheme of ageing, that may be the most rebellious act of all.
If you’d like to put any of this into practice, we’re based in East Horsley and we’d love to help. [Get started here.]
Be The First To Comment