
ARTICLES

The GLP-1 Tightrope: Why Your Muscles are theNon Negotiable Safety Net
Ally Taylor
16/03/2026

AN ARTICLE BY ALLY TAYLOR
Let’s talk about the elephant in the room: or rather, the elephant that has suddenly vanished from the
room thanks to a weekly prick in the thigh.
If you’ve spent any time chatting to people around Surrey lately, you’ve heard the whispers. It’s the
“skinny jab,” the “miracle shot,” the “Hollywood secret.” GLP-1 agonists (think Ozempic, Wegovy,
Mounjaro) are currently doing for weight loss what the internet did for awkward dating: changed the
landscape forever.
For many, these medications are a genuine lifeline which has the power to change lives. The point of this post isn’t to clutch pearls about medication. It’s to zoom in on the physiology that decides whether your weight loss turns into health… or just a smaller body with fewer “spare parts” to cope with real life.
Enter: Gary.
Gary is a fictionalised version of about six people I’ve spoken to this month. He’s 58, lives a stone’s throw from our studio in East Horsley, Surrey, and has spent the last decade fighting a losing battle with his midsection and a penchant for Italian reds. Three months ago, Gary started a GLP-1. The results? Spectacular. The “food noise” in his head: that constant internal monologue debating whether he should have a second biscuit: has been muted. He’s down two trouser sizes. His GP is thrilled.
But Gary? Gary also has questions (the best kind of client, honestly).
He’s a bit more tired than expected. His golf swing feels like he’s trying to move a lead pipe through treacle. And he’s noticed something odd: he’s lighter, but not necessarily stronger. So instead of Gary being a cautionary tale, he becomes what lots people on these meds eventually become: a sensible adult who realises the jab is a tool… and tools work best with a whole toolbox and a plan!
Gary is currently walking a tightrope. The safety net isn’t “more willpower.” It’s muscle.
The “Lean Mass Tax” You Didn’t Agree To
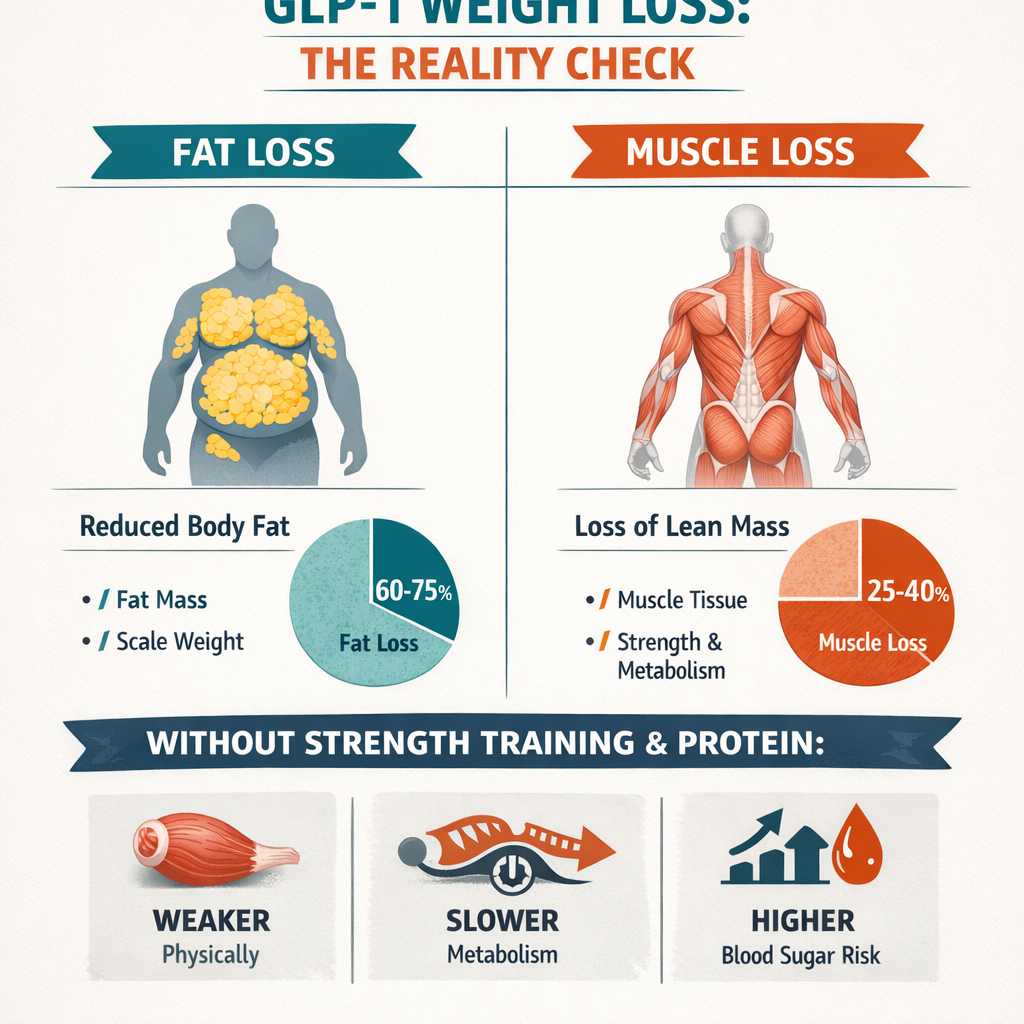
Here is the bit that doesn’t make it into the glossy “before and after” TikToks. When you lose weight quickly via appetite suppression (a big part of how GLP-1s help), your body doesn’t exclusively burn fat. It pulls from multiple compartments: fat mass, glycogen/water… and lean mass (which includes skeletal muscle, organ tissue, and some connective tissue).
In obesity drug trials, a meaningful chunk of total weight lost can come from lean mass if lifestyle isn’t deliberately managed. In the big GLP-1 programmes (e.g., STEP trials for semaglutide and SUSTAIN for type 2 diabetes populations), analyses commonly show that roughly 25–40% of weight lost can be lean mass in the absence of an intentional resistance training + protein strategy. To be super clear, this is not because the medication is “bad,” this is a side effect of all rapid weight loss; whether diet, medication or surgical. This is because physiology is ruthlessly efficient: if you’re not signalling “keep this muscle,” your body won’t treat it as precious.
Think about that for a second. If Gary loses 20kg, somewhere between 5–8kg could be lean mass. That’s potentially a huge reduction in the very tissue that helps keep him independent, stable, and resilient as he ages. And if you’re in your 50s and 60s, you’re already dealing with age-related muscle loss (sarcopenia) in the background. Rapid weight loss can accelerate the problem unless you build the guardrails.
Muscle: Your Metabolic Sink (and Why That Matters More Than Your BMI)
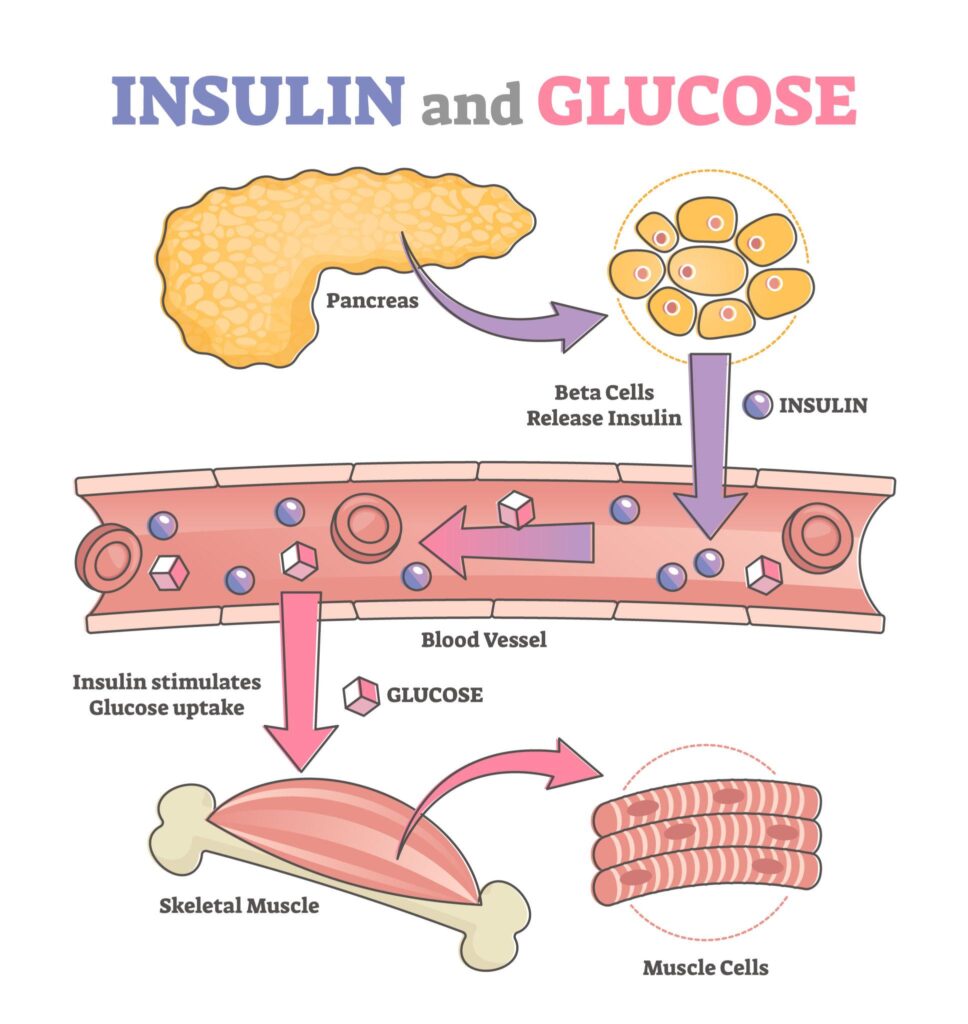
Why should Gary care? Because muscle isn’t just for aesthetics or “being strong.” Skeletal muscle is one of the biggest sites of glucose disposal in the body. After you eat, around ~80% of postprandial glucose uptake happens via skeletal muscle (largely insulin-mediated). That’s the “metabolic sink” concept in plain English: muscle is where a lot of the incoming fuel gets parked and processed.
Lose a chunk of that sink and you don’t just get smaller; you get less metabolically flexible. You have less tissue available to soak up glucose, less storage capacity for carbohydrate, and often a worse ability to transition between fuels smoothly.
So yes, muscle is “expensive tissue” and it burns energy just existing (even while you’re on the sofa watching Bridgerton for the fourth time). But the bigger deal for long-term health is that it’s a key player in blood sugar control and metabolic resilience.
When Gary loses lean mass without a plan, he’s not just shrinking his body; he’s shrinking his buffer.
The “Food Signal” Coming Back Online (and Why Habits Are the Exit Plan)
Here’s the part of the story Gary has thought about (because Gary is now doing this properly): what happens when the dose is reduced or the medication is stopped? Most people don’t plan to stay on these injections forever. Maybe it’s the cost, maybe it’s the side ef fects, or maybe they just reach their goal and want to maintain without it.
Data tracking what happens after GLP-1 therapy is stopped shows a pattern that’s… annoyingly human. Weight regain is common. Appetite tends to reassert itself. The medication quietens the “food noise,” but it doesn’t magically install new routines in your diary or protein in your fridge.
Imagine you’ve been wearing earplugs for a year. When you take them out at a rock concert, the noise is deafening. That can be what appetite feels like post-medication. And if you’ve also lost a meaningful amount of lean mass along the way, you’re trying to maintain your results with:
• a louder appetite signal, and
• a smaller metabolic sink.
That combination doesn’t mean you’re doomed. It just means the long game is built on behaviours, not just biology.
The Real Safety Net: Strength Training (Surrey Edition)
If you’re on a GLP-1, or thinking about it, I’m here to give you the blueprint that makes the medication work with your body rather than quietly dismantling it behind your back. You need a safety net. And that net is built with two things: strength training and protein.
At Amovida, we specialise in intelligent personal training that’s tailored, calm, and non-intimidating (no gym-gym energy, no performative grunting, no “punishment workouts”). Why? Because for many people: especially those wanting personal training over 50: consistency beats chaos every time.
Here’s the “why” behind the training:
1. Preserve (or regain) lean mass – Resistance training tells your body: “This muscle is useful. Keep it.” That shifts the composition of weight loss so you’re more likely to lose fat mass rather than haemorrhage lean mass.
2. Reduce the risk of sarcopenic obesity – Sarcopenic obesity is the worst-of-both-worlds scenario: you lose muscle while keeping fat (or you lose both, but the proportion of body fat ends up higher because muscle dropped so much). You can look “smaller” but be metabolically worse off and physically less capable. Strength work is one of the most direct countermeasures we have.
3. Keep joints, posture, and movement options – As bodyweight changes quickly, people often move less (sometimes because they’re tired, some times because they’re eating less, sometimes because life is life). We build strength with mobility so your new body still feels like a place you can live comfortably.

The Protein Gap (Yes, Even If You “Aren’t That Hungry”)
One of the sneakiest problems with GLP-1s is also one of the reasons they work: you’re less hungry, so you eat less. Brilliant. But if you eat less without strategy, protein is usually the first thing to quietly disappear (because toast is easier than chicken). That creates what I call the protein gap: you’re in a calorie deficit and you’re under-eating the key nutrient that protects muscle during weight loss.
If you’re using a GLP-1 and you want the best chance of keeping lean mass, high protein intake is the non-negotiable partner to the jab. A commonly used evidence-based target for active dieting phases is roughly ~1.6–2.2g of protein per kg of body weight per day (individual needs vary, and medical conditions matter, so get personalised advice if you need it).
No, you don’t have to live on protein shakes and sadness. But you do need a plan: • anchor meals around a quality protein source
• spread it across the day (not a single heroic chicken event at 8pm)
• make it “easy protein” when appetite is low (Greek yoghurt, eggs, fish, whey, cottage cheese, tofu/ tempeh, lean meats)
Gary’s biggest win wasn’t “trying harder.” It was realising that if appetite is blunted, planning becomes the replacement for hunger cues.
Exercise Isn’t “Extra Work.” It’s the Insurance Policy.
The jab can help you lose weight. Strength training helps you keep the machinery that makes maintenance possible. Think of it like this: medication can be the accelerator for fat loss. Training is the insurance policy for what happens when the dose is tapered, paused, or stopped. It’s the thing that keeps your body capable when biology becomes less… cooperative.
And the best version of this isn’t hero workouts. It’s a sustainable routine you can repeat in real life, in Surrey, with your job and your knees and your schedule.

Don’t Just Be Smaller. Be Stronger.
Gary came to see us last week. He’s still on his medication, but his focus is different. He’s no longer obsessed with the number on the scale going down; he’s obsessed with the number on his deadlift going up.
He’s eating more protein. He’s working on his strength. He’s feeling “tight” again: in a good way. His golf swing is coming back.
If you’re in East Horsley (or nearby in Surrey) and you’ve started your own GLP-1 journey, don’t leave your muscles behind. Don’t be the person who hits their goal weight only to realise they can’t carry their own groceries up the stairs.
Come and see us at Amovida. Whether you’re looking for a personal trainer who understands the nuances of aging and metabolic health, you want evidence-led strength training, or you’re specifically after personal training for over 50s, we’ve got you.
The “miracle” is in the medicine, sure. But the magic: the long-term, sustainable, “I feel bloody fantastic” magic: is in the muscle.
Let’s build yours.
Visit us at Amovida to start your journey
Be The First To Comment